

Labcorp Plasma Detect ID MRD Test for Non‑Small Cell Lung Cancer (Stage I-IIIA)
Labcorp Plasma Detect ID MRD test for non‑small cell lung cancer (stage I-IIIA) defines a personalized, tumor-informed MRD signature by analyzing whole exome sequencing (WES) of tumor DNA and matched germline DNA collected at the baseline timepoint. Based on this analysis, a patient’s tumor specific panel of 18–50 variants is developed to detect circulating tumor DNA (ctDNA) in blood samples, both at the baseline and monitoring timepoints.

Unmet clinical need for molecular residual disease (MRD) testing in
non‑small cell lung cancer (NSCLC)1-4
High relapse rates despite curative therapy
Up to 10-55% of patients with resected stage I-IIIA NSCLC relapse within 5 years
Limitations of standard surveillance tools
Standard imaging (CT/PET scans) typically detects recurrence only after subclinical disease is present
Lack of sensitivity for subclinical disease
After curative-intent surgery or chemoradiotherapy, subclinical disease cannot be reliably measured with existing surveillance modalities due to lack of sensitivity for early molecular relapse detection
Opportunity for earlier intervention
TRACERx data3 demonstrate that presence of ctDNA can identify molecular recurrence months before radiographic progression (median lead time 3+ months), enabling timely intervention
Why choose Labcorp Plasma Detect ID MRD
in NSCLC (stage I-IIIA)
-
Highly sensitive MRD test*: Detects ctDNA at levels as low as 0.005% (50 PPM)
-
Proven analytical precision*: Demonstrates >99.9% sensitivity and >99.9% specificity at the reported limit of detection
-
Early recurrence signal: Provides a median lead time of 3+ months before clinical or radiologic evidence of recurrence 3

*Sensitivity and specificity data derived from an internal analytical validation study
Clinical evidence for Labcorp Plasma Detect ID MRD in NSCLC (stage I-IIIA)3
Postoperative ctDNA‑positive result is associated with worse clinical outcomes
Patients with detectable ctDNA within 120 days after surgery had a 5.3‑fold higher risk of death and a 6.8‑fold higher risk of disease recurrence compared with those who were ctDNA‑negative, underscoring its prognostic value for guiding post‑surgical management.
Early molecular detection with months of lead time over standard‑of‑care surveillance tools
ctDNA detection by the Labcorp Plasma Detect ID MRD test provided a median of 119 days (3+ months) before clinical or radiological evidence of recurrence.
High positive predictive value for relapse
A postoperative ctDNA‑positive result predicted relapse with a 93% positive predictive value.
Surveillance improves sensitivity beyond a single timepoint
Longitudinal ctDNA monitoring every 3–6 months increased sensitivity, detecting 20% more relapses than single‑timepoint analysis alone.
Sample requirements for baseline and monitoring timepoints
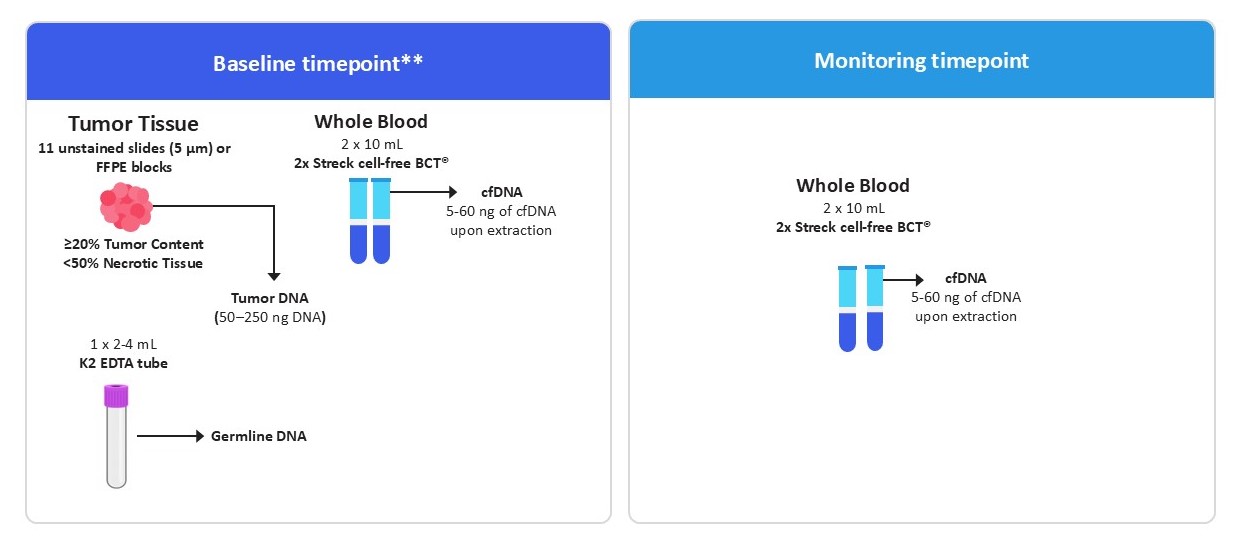
Baseline results are delivered in 35-42 days
Monitoring results are delivered in 7-14 days
**Both tissue and blood samples are required for the baseline analysis.
How to order
To begin testing, first order the Labcorp Plasma Detect ID specimen collection kit.
After the kit order is placed, the test may be ordered using a test requisition form, through the Labcorp Link portal, or via your EHR using your Labcorp clinical account number.
Your Labcorp Oncology representative will work with you to implement the ordering method that best fits your clinical workflow.
Clinical support
Our team of pathologists and oncologists is available to support you and your practice:
- Email: [email protected]
- Phone: 800‑366‑7230
- Fax: 919‑361‑7296
Why partner with Labcorp for your oncology testing needs
Streamline your workflow with MRD tests that can be ordered from a broad cancer diagnostic portfolio
Comprehensive
A full spectrum of oncology and clinical testing across the continuum of care: spanning screening, risk assessment, diagnostics, prognostics, monitoring, and surveillance, including germline and somatic testing with tissue- and liquid-based next-generation sequencing for comprehensive genomic profiling
Connected
Seamless ordering & reporting
Contracted
Broad payer coverage
Convenient
Nationwide access to patient service centers for blood draw and shipment
Additional MRD tests
Test disclaimer
This test is a laboratory-developed test (LDT) performed by Labcorp (Metropark site, NJ), which is accredited by the College of American Pathologists (CAP) and certified under the Clinical Laboratory Improvement Amendments (CLIA). It has not been cleared or approved by the U.S. Food and Drug Administration (FDA).
References
- Rajaram R, Huang Q, Li RZ, Chandran U, et al. Recurrence-free survival in patients with surgically resected non-small cell lung cancer: a systematic literature review and meta-analysis. Chest. 2024;165(5):1260-1270. doi:10.1016/j.chest.2023.11.042
- Pellini B, Chaudhuri AA. Circulating tumor DNA minimal residual disease detection of non-small-cell lung cancer treated with curative intent. J Clin Oncol. 2022;40(6):567-575. doi:10.1200/JCO.21.01929
- Abbosh C, Frankell AM, Harrison T, Kisistok J. High resolution phylogenetic ctDNA tracking predicts relapse risk and metastatic dissemination patterns in early-stage lung cancer. Nature. Published online April 2023.