

Labcorp Plasma Detect Genome MRD for Colon Cancer (Stage III)
Labcorp Plasma Detect Genome MRD is a tumor‑informed MRD assay that uses whole‑genome sequencing to detect circulating tumor DNA (ctDNA) in plasma at baseline and monitoring timepoints.

Unmet clinical need for MRD testing in stage III colon cancer1-4
High relapse rates despite curative therapy
Up to ~30-35% of patients with stage III colon cancer experience disease recurrence within 5 years after curative-intent treatment
Limitations of standard surveillance tools
Conventional imaging (MRI, CT scan, PET scan) and serum biomarkers (CEA) typically detect recurrence only once subclinical disease is present, limiting their utility for early recurrence detection
Lack of sensitivity for subclinical disease
Following surgery and/or adjuvant chemotherapy, subclinical residual disease cannot be reliably measured with current surveillance modalities, leaving a gap in early recurrence detection
Opportunity for earlier intervention
ctDNA MRD tests have demonstrated the ability to identify molecular recurrence months before radiographic progression, offering a window for earlier intervention
Why choose Labcorp Plasma Detect Genome MRD in colon cancer (stage III)
-
Whole-genome MRD surveillance: Leveraging whole-genome sequencing (WGS) for longitudinal monitoring, capturing a broad molecular landscape. A median of approximately 5,000 patient‑specific tumor variants are tracked
-
Fast turnaround time for tumor-informed MRD testing: 14 days for baseline test results and 7 days for monitoring test results
-
High analytical sensitivity*: Utilizes WGS of tumor DNA, White Blood Cell DNA, and WGS of cfDNA to detect MRD at low levels with confidence with a sensitivity of 0.005% ctDNA content (50 PPM) and a specificity of 99.4%

*Sensitivity and specificity data derived from an internal analytical validation study
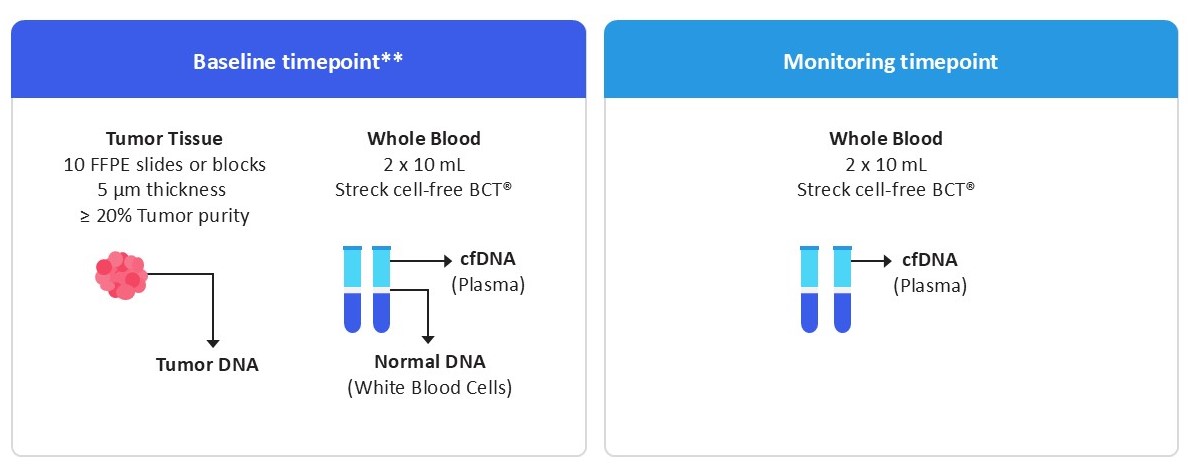
Sample requirements for baseline and monitoring timepoints
Baseline results are delivered in 14 days
Monitoring results are delivered in 7 days
Baseline timepoint:
- Tumor tissue: Submit 9 pre‑cut unstained slides from paraffin block cut at 5 µm thickness and 1 matching H&E reference slide, or an FFPE tissue block. Tumor surface area ≥ 4 mm²; tumor content ≥ 20% preferred.
- Peripheral blood collection: Two 10 mL Streck cell‑free BCT® tubes drawn 1 week to 2 months post‑surgery or post‑adjuvant therapy.
Monitoring timepoint:
- Peripheral blood collection: Two 10 mL Streck cell‑free BCT® tubes.
Labcorp Plasma Detect Genome MRD workflow advantages
Labcorp Plasma Detect Genome MRD eliminates the need for custom panel design, resulting in a faster turnaround time for results compared to tumor-informed bespoke tests that require custom panel design for each patient.

Ordering and reporting process
- Order your kit: Request a specimen collection kit through [email protected].
- Place your test order: Order via paper TRF or Labcorp LINK® or EHR using Labcorp clinical account
- Ship specimens: Use provided FedEx label to send specimen kits to Labcorp CMBP lab
- Receive Results: Access results via Labcorp LINK®, EHR, secure email, or fax
Your Labcorp Oncology sales representative will partner with you to implement the method that works best for your clinical workflow.
Clinical support
Our team of pathologists and oncologists is available to support you and your patients:
Email: [email protected]
Phone: 800-366-7230
Fax: 919-361-7296
Additional MRD testing options
Test disclaimer
This test is a laboratory-developed test (LDT) performed by Labcorp, which is accredited by the College of American Pathologists (CAP) and certified under the Clinical Laboratory Improvement Amendments (CLIA). It has not been cleared or approved by the U.S. Food and Drug Administration (FDA).
References
- van den Berg I, Coebergh van den Braak RRJ, van Vugt JLA, et al. Actual survival after resection of primary colorectal cancer: results from a prospective multicenter study. World J Surg Oncol. 2021;19:96. doi:10.1186/s12957-021-02207-4
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Schirripa M, Lenz HJ. Biomarker in colorectal cancer. Cancer J. 2016;22(3):156-164. doi:10.1097/PPO.0000000000000190
- André T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350(23):2343-2351. doi:10.1056/NEJMoa032709